Advice on my daughter's health
by Sue
(Sydney, Australia )
My daughter is 26yo, since starting menstruating she has had episodes of excruciating lower right flank pain, with full on shock symptoms - clammy, grey skin, feeling faint etc. This started when we were overseas and she was 13yo and almost ended up in an ER in Moscow, fortunately a friend who is a Doctor suggested some Cal-Mag drink and rest, and she recovered after 1-2 days. Again when she was 20yo and I was not with her, she had another incident and ended up in a fetal ball in the corner of her office, again grey, clammy skin and in full-on stabbling pain again in the right lower pelvic area. She did all the tests, USS, bloods, etc and the diagnosis was a ovarian cyst had burst, and all they could find was some sort of residue and then a large cyst on the left. We are talking specialists in one of the most well-thought of clinics in Sydney. She continued with cyclic pain in the same region, when it happened she lost appetite, felt nauseous, was off work for 3-4 days. She also had acne during the pre-menstural days, and some dark hair growing on her upper lip. She usually has a sub-normal temp and low BP when this is happening.
Earlier this year she had another episode, we had been dealing with the cyclic problems with Magnesium, Vit C IV, exercise and a form of Assists that helped but did not cure.
When she had this major episode in Feb-March I decided this was it, with the help of a holistic GP in New Zealand who has helped me and our local GP who was determined to get to the bottom of this we started a round of specialists and USS and so on. Even went to ER room when the pain was 7-8 on the scale, still nothing. One Gynaecologist confirmed an earlier diagnosis of PCOS, another holistic GP found her thyroid had gone very high and was refusing further IVs until she went to a thyroid specialist (NZ GP said no way this was not the problem), her prolactin skyrocketed and she was off work for days. Pelvic USS found adnexal mass - probably ovarian cyst, holistic GP thought maybe chocolate cyst bleeding causing the pain, appendicitis was looked for and still nothing. Finally I got her to a very prominent Gynaecologist in Sydney - Prof Michael Cooper. He did an internal USS - earlier she had refused to do this as it was too painful. He said almost immediately - mullerian anomaly - explained what he thought and sent her for 3D USS which confirmed this as a non-communicating right uterine horn - and endometriosis in the area. His suggestion remove the anomaly as it posed a very real life-death risk if she got pregnant in that horn, and get the endo out and then into a full exercise, dietary and lifestyle improvement to sort the reproductive area out and be able to fall pregnant. Holistic Dr in NZ meanwhile had me on progesterone for my situation (different story) and suggested my daughter go on it too. She started on the cream and better diet (organic chicken/meat, vegges and gluten free) which helped and she started losing weight and feeling better. She went ahead with the operation to remove the anomaly and the Gynae found a large amount of endo in the cul-de-sac covering bowel and bladder as well as pulling the bowel up into the uterus. He was an extensive operation and she is now recovering under directions from our GPs (Sydney and NZ). She still has acne and dark hairs and while she is losing weight and eating better, exercising more and there was no evidence of PCOS in the operation, I want to ensure her recovery is a full one. My questions are - 1) what causes mullerian anomalies occurring - it was from me as it forms in the early stages of the fetus - and before I discovered I was pregnant with her I had had a major incident with mouth ulcers and physical exhaustion - and 2) what program does she need to be on now in relation to progesterone and other related supplements? She does not plan to get pregnant for a while and Gynae recommendation is a Mirena IUD device which she wont be doing. And 3) were we right to go ahead and do the op or was there a better more holistic handling we should have done first. My prime concern was the amount of pain and discomfort she was in almost chronically despite using magnesium, Vit D and other supplements to handle. She does not take painkillers and never has in her life - expect twice during these incidents mentioned above.
I want her to make a full and complete recovery so I am coming to you as I have been reading your website and I like your approach and solutions you give the other ladies.
Comments for Advice on my daughter's health
|
||
|
||
|
||
|
||
|
||
|
||
|
||
|
||
Do you have a progesterone deficiency?
This free questionnaire
will tell you in 5 minutes.
Just enter your email
and click the button...
Subscribe to our Progesterone Therapy Newsletter
It's free and will bring you important new information on progesterone therapy, related health matters and discount specials.
Do you have a
question or concern?
See what's being discussed, ask for help, give your thoughts or experiences, or just browse...
or
Recent Articles
-
Beyond PCOS: How PMOS Better Explains The Condition
May 19, 26 08:00 AM
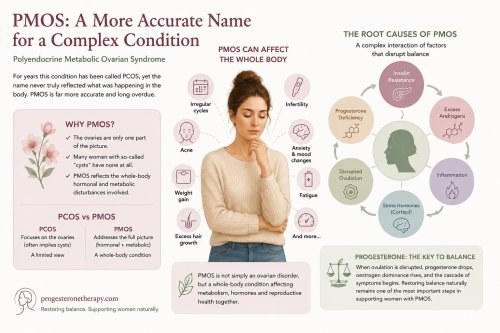 For years this condition has been called PCOS, yet the name never truly reflected what was happening in the body. The ovaries are only one part of the picture. Many women with so-called “cysts” have n…
For years this condition has been called PCOS, yet the name never truly reflected what was happening in the body. The ovaries are only one part of the picture. Many women with so-called “cysts” have n… -
PMOS
May 15, 26 09:51 AM
Polyendocrine Metabolic Ovarian Syndrome (PMOS) -
Contraceptives
May 09, 26 11:11 AM
 Contraceptives are now ubiquitous, reaching even the most remote rural communities. But their widespread use raises an important question—at what cost to a woman’s health? All drug-based contraceptive…
Contraceptives are now ubiquitous, reaching even the most remote rural communities. But their widespread use raises an important question—at what cost to a woman’s health? All drug-based contraceptive… -
Honouring Value: Upcoming Natpro Price Changes
Apr 19, 26 09:34 AM
 We deeply value your trust and loyalty as part of the Natpro community. Over the past 30 years, we have worked hard to keep Natpro’s pricing stable, ensuring the highest quality natural progesterone c…
We deeply value your trust and loyalty as part of the Natpro community. Over the past 30 years, we have worked hard to keep Natpro’s pricing stable, ensuring the highest quality natural progesterone c… -
Hot Flushes, why they happen and how to get relief
Apr 08, 26 04:37 AM
 Hot flushes are the body’s attempt to regulate temperature, a natural response when it senses an imbalance. The skin, being the body’s main defence against overheating, responds with flushing and swea…
Hot flushes are the body’s attempt to regulate temperature, a natural response when it senses an imbalance. The skin, being the body’s main defence against overheating, responds with flushing and swea…
Natural
progesterone cream
Your language
Translate this website
into your language
Is this the future
of medicine?
Home | Contact | Newsletter | Index of Symptoms | News | Progesterone cream | Privacy policy | Blog | About | FAQ
Disclaimer:
Although this web site is not intended to be prescriptive, it is intended, and hoped, that it will induce in you a sufficient level of scepticism about some health care practices to impel you to seek out medical advice that is not captive to purely commercial interests, or blinded by academic and institutional hubris. You are encouraged to refer any health problem to a health care practitioner and, in reference to any information contained in this web site, preferably one with specific knowledge of progesterone therapy.