How to use progesterone cream
There are as many instructions on how to use progesterone cream as there are brands.
There are 11 Delivery systems...
- Injections
- IV transfusions
- subcutaneous implants
- suppositories/pessaries
- vaginal tablet
- troches/lozenges
- buccal drops
- oral caps
- gels
- oils and creams
Creams are regarded by most as the best option, certainly the best for men. They can contain liquid paraffin, parabens, phenoxyethanol, sodium lauryl sulphate, propylene glycol, fragrances, artificial colours and PEG emulsifying waxes, these can contain dioxane a known carcinogen. For more information about toxins in skin creams see Skin Deep.
The strength of the creams vary from 1.5% to 10%. This means a 1.5% cream contains 15mg progesterone per gram (g) or millilitre (ml). A 10% cream contains 100mg per gram (g) or millilitre (ml).
So dependant on the amount of progesterone required, the amount of cream must be taken into account.
The progesterone in a cream is absorbed well, and has been found to be as effective as injections and to enter circulation rapidly.
Creams have an advantage over all the other systems. No special method or applicator is needed to apply a cream, there's no discomfort in using it as in some delivery systems, in fact it often soothes the problem quickly. It can be applied within seconds, on the run if need be.
A progesterone cream can be used anywhere on the body, it does not have to be applied to the thin skinned areas only. The skin comprises 95% kerotinocytes, these have ample progesterone receptor sites. Even hair follicles absorb progesterone well. For more information see Progesterone misconceptions.
Please note that progesterone will help if the problem is caused by a lack of it, or if excess oestrogen is present. But there are many other factors involved too.
For instance a lack of vitamin D reduces the benefits of progesterone, please have a test done. Large meals, dark gloomy days, winter, high adrenaline levels, excess blood glucose, a high amount of phytoestrogens in the diet, HRT and the contraceptive pill, all affect it adversely.
Please check the Nutrition page for advice on food.
Men
Using progesterone is very easy for a man as he has no cycle. Therefore it can be applied daily. It's best to apply it twice a day, more frequently if symptoms are severe.
Use between 10-100mg/day progesterone, more if severe symptoms are experienced.
Levels over 1200mg/day are given to men who have suffered a Traumatic Brain Injury.
Men secrete <3.18 nmol/L (<1 ng/ml) progesterone daily. For more information on levels see Hormone Testing.
Women
The number of instructions given, the apparent complications of using it, and the misinformation, has caused many hundreds of women to abandon using it.
The main consideration above all else is use enough to reverse any adverse symptoms.
Too little and it merely exacerbates them.
The amount to use is not dependant on a given 'dose' or on size, weight, height or sex, but on symptoms.
The typical 20-40mg/day that is recommended does not raise levels to that found in the luteal phase. One study found that using 40mg/day...
"...only low plasma progesterone levels were found (median 2.5 nmol/l)"
The ranges for the luteal phase are 15.9 - 63.6 nmol/L (5 to 20 ng/ml). Men secrete <3.18 nmol/L (<1 ng/ml). For more information see Hormone Testing.
For general use and to reverse mild symptoms 100-200mg/day progesterone is needed. If severe problems are experienced 400-500mg/day are needed.
Once symptoms have passed the amount should be reduced very slowly, until the optimum is found.
It's essential to reduce over a few weeks
to prevent adverse symptoms returning.
It should be used a minimum of twice a day as levels begin dropping after about 13 hours. But in severe cases, application can be hourly.
When first starting progesterone it can disrupt the cycle. Periods can be either earlier or later than normal. This is nothing to be concerned about, the normal cycle length will assert itself within a few cycles.
If spotting only occurs, continue using the progesterone until bleeding starts.
If a full period occurs stop using the progesterone, and begin it again 12-14 days before the next period. For further explanation on this see under Normal Cycle Lengths below.
Bleeding can be heavier in the first few cycles, also nothing to be concerned about. This is old lining which has not been shed previously.
The four phases of a woman's life
- Pre-pubertal
- Reproductive
- Peri-menopause with dropping fertility levels
- Menopause
Progesterone is safe to use in all four phases.
Pre-pubertal phase
It's given to pre-term male and female infants with respiratory distress syndrome. It's effective for calming, and for any sleep issues in babies and children. Babies have been bathed in it for 9 months of their lives prior to birth.
Progesterone is the only hormone that does not adversely affect a male or female baby or child. So if some should rub off an adult using it, no harm will come. Unlike testosterone or oestrogen, which cause serious side effects in a male or female baby or child.
If progesterone is used on an infant or child, very little is needed:
1mg of progesterone or a pin head amount of cream can be applied to infants,
Older children use 5-10mg which is between 0.2ml to 0.3ml of cream
It only needs to be used for easing the child over a rough patch.
It helps with adverse symptoms experienced prior to puberty, and any found while going through puberty. Menstruation starts about two years after puberty begins and is known as menarche.
These two years can bring mood swings, temper tantrums, defiant behaviour, skin outbreaks and more. Oestrogen and testosterone levels are rising, but it's not until menarche occurs and with it ovulation, does progesterone production begin.
100-200mg/day progesterone should be used, dependant on symptoms.
As there is no cycle to follow the progesterone can be applied daily
until a cycle starts.
Reproductive phase
This lasts from menarche to peri-menopause when fertility starts to drop. A normal cycle length varies from 21 days to 35 days, 28 days being the average. This is the reason that manufacturers of Contraceptives and HRT pack their product in twenty eight day batches.
Cycles outside this range are generally regarded as abnormal. For more information on this see the pages on Menstruation and PCOS.
All women, irrespective of their cycle length, ovulate 12-14 days before bleeding.
This phase of the cycle is known as the luteal or secretory phase.
Progesterone should be used during the luteal phase, ie from ovulation to bleeding, to supplement any deficiency.
The deficiency can be caused by a defective luteal phase, or anovulatory cycles. These begin round about age 35, which is when many women find their PMS symptoms become worse.
100-200mg/day progesterone should be used, more if symptoms are severe.
Normal Cycle Lengths
Everyone, including the medical profession, assumes a normal cycle length is always 28 days in all women. This is simply not the case.
It varies between 21 to 35 days, which makes 28 days the average only.
There is a fundamental error in advising women to start using progesterone on day 14. This is only appropriate for women with a 28 day cycle.
If a woman has a 21 day cycle, starting on day 14 would mean she starts using progesterone a week after ovulation. She would then only use progesterone for 7 days before bleeding began.
Likewise a woman with a 35 day cycle would begin progesterone a week before ovulation, which would effectively stop it. She would then use progesterone for 21 days.
Progesterone should always be used from ovulation,
for the last 12-14 days of the cycle.
Or if wishing to fall pregnant, it can be started during the 50 hour surge which occurs prior to ovulation.
Progesterone can be used while on drug based Contraceptives. It should be used when taking the second half of the packet.
Progesterone is safe to use with any drug, there are no contraindications.
Peri-Menopause
This normally begins 5 to 10 years before menopause. As a rough guide, women tend to go into menopause round about the same age as their mothers. There's no significant change when entering peri-menopause, such as the start of bleeding in puberty. Or the stopping of bleeding in menopause.
Many women have no symptoms at all, but many do, some quite severe. Progesterone levels are now dropping, and continue dropping at an ever faster rate. This is due to the increased frequency of anovulatory cycles.
Roughly one to two years prior to menopause cycles can become very erratic. Every two weeks, or at three month intervals, there is no telling when bleeding will occur. This can vary from spotting, to a normal period, to flooding.
100-200mg/day progesterone should be used, more if symptoms are severe.
Once cycles become erratic, and impossible to follow, it's best to stop following the cycle and use progesterone daily, through any bleeding. It is safe to do so. For more information see Progesterone misconceptions. Ironically no caution is given to women who take contraceptives continually, some of which are progestin only.
Menopause
This begins on average at age 51. It's normal to wait a year before judging menopause has begun. Many women think their problems will be over once in menopause, but this is often not the case.
Ovulation has now ceased, ovarian production of progesterone and oestrogen has stopped. But fat cells continue secreting oestrone, the menopause oestrogen, until death. Unfortunately there is no compensatory secretion of progesterone.
Many women have their oestrogen levels tested and are told it is low. But it's oestradiol which is tested for, the pre-menopause oestrogen, never oestrone. Oestradiol should be low, it varies from 0-30pg/ml (0 - 110.13 pmol/L), see the page on Hormone Testing for more information.
100-200mg/day progesterone should be used, more if symptoms are severe.
As there is no cycle to follow use progesterone daily. Many women are advised to take a break, but it's not necessary. For more information see Progesterone misconceptions. Ironically no caution is given to women who take HRT continually.
Women who begin using progesterone for the first time once in menopause can experience one period, rarely two. This is nothing to be alarmed about. Over the course of the proceeding months or years the small amount of oestrogen being secreted by fat cells is enough to build or thicken the lining. The progesterone is effectively cleaning out the uterus.
The bleeding more often than not occurs within the first year of menopause, but it has been known for women 12 years into menopause to have a period when first using progesterone.
Hormonal variations chart in both men and women..

More Information on how to use progesterone cream
Pregnancy... How to use progesterone before conception and during pregnancy is explained on this page. There's is an explanation of a defective luteal phase and how to extend it. Plus information on the surge of progesterone that comes from the brain prior to ovulation, and how to use progesterone to enhance ovulation and implantation.
Contraception... Progesterone can be used as a contraceptive. It has none of the adverse side effects the drug based contraceptives can have.
It should be started 3 to 8 days or more before ovulation depending on the cycle length. This will stop the oestrogen surge which occurs 2-5 days before ovulation. This surge of oestrogen is necessary to complete the final step before ovulation. There's more information about the mid-cycle surge of hormones on the pregnancy page.
A study of progesterone contraception found a failure rate of 2.66 pregnancies per 100 women, which compares well with other methods. Please be aware that stress drops progesterone levels, so protection drops. Increase the amount used to cover the stressful time, or use a temporary alternate method. There's more information on this page.
Amounts of 100-200mg/day should be used.
It should be continued until bleeding occurs when it should be stopped. Resume using it again as outlined above.
Adverse symptoms... If symptoms are severe, it's advisable to use progesterone daily for the entire month, using it through any bleeding. Follow this procedure for 2-3 months or until stable. This ensures progesterone becomes the dominant hormone. Each time a break is taken for the follicular phase, ie from bleeding to ovulation, oestrogen rises again, and adverse symptoms return.
Once stable the cycle can be followed again. ie when the next period occurs, stop using the progesterone for the follicular phase, and resume again at ovulation. If this is not known, start again 12-14 days before bleeding.
For general use it's not necessary to know when ovulation occurs, beginning 12-14 days before bleeding is sufficient. But if pregnancy is the aim, it is necessary to know when ovulation occurs. The pregnancy page explains this in detail.
Very heavy, and/or continual bleeding... see the Menstruation page for information.
Stress... drops progesterone levels sharply, so adverse symptoms can return. The reason for this is cortisol, the stress hormone, is made from progesterone. The stress response is a survival instinct, so the body will use any available progesterone to convert it into cortisol to overcome the stress, be it acute or chronic, good or bad. Progesterone should be increased over any stressful time.
Oestrogen Dominance... This is a term coined to describe adverse symptoms which occur when first using progesterone. It generally occurs if 20-40mg/day progesterone is used. Dr Dalton's patients never experienced it as she gave them amounts varying between 400-800mg/day.
It also occurs in the early days of pregnancy with rising progesterone levels. If progesterone doesn't rise fast enough nausea, headaches, tiredness, high blood pressure and more can occur. The same symptoms can occur in the last month or so of pregnancy, when progesterone should be at it's peak. This can lead to pre-eclampsia.
It can also occur when first using progesterone, when increasing it, when decreasing it or stopping it. Or when changing brands of progesterone without taking into account the amount of progesterone in the product.
Many blame progesterone and reduce the amount they're using, ironically this does help. It's now no longer stimulating oestrogen, but defeats the purpose. Which is to suppress the excess oestrogen causing the adverse symptoms in the first place.
To prevent it happening progesterone should be increased. Ideally, high amounts should be used initially to prevent it occurring.
Adverse symptoms only occur when
the ratio of progesterone to oestrogen becomes unbalanced.
They can occur from the last few days prior to and during bleeding, and are due to dropping progesterone levels, generally referred to as progesterone withdrawal. The medical term catamenial is used to describe them, from the Greek word for menses or menstruation. A more common term is PMS.
They can also occur just prior to and during ovulation. And they can occur during the entire luteal phase. Plus of course they can occur in the early days of pregnancy, throughout it's duration, or after birth.
In every case it's caused by a shortage of progesterone in ratio to oestrogen.
The higher the oestrogen, the lower the progesterone, the worse the symptoms.
Some of the severer symptoms which can occur are...
- migraines
- heart palpitations
- seizures
- anxiety and panic attacks
- depression
- asthma attacks
- collapsed lung
- post natal depression and psychosis after birth
If any of these symptoms are experienced prior to using progesterone, it's essential to use very high amounts to prevent worsening of symptoms due to oestrogen dominance, i.e. 400-500mg/day.
Oestrogen rises exponentially 2-5 days before ovulation. Progesterone should surge during these days too. This surge comes from the brain, and has nothing to do with the rise in progesterone after ovulation. If this surge does not take place, oestrogen will be dominant and severe symptoms can be experienced.
Oestrogen peaks mid-luteal phase. Progesterone should too. But if there's a failure in the corpus luteum to secrete sufficient progesterone during the luteal phase, or if ovulation does not take place, severe symptoms can be experienced throughout the luteal phase.
If the luteal phase proceeds normally, ie there is the pre-ovulatory surge in progesterone, ovulation takes place and the corpus luteum secretes sufficient, no adverse symptoms will be experienced.
But the rapid drop in progesterone levels the few days before bleeding are enough to cause adverse symptoms in many women.
The following pages give more information on other adverse problems...
From running Saliva Tests it's been found the ratio of progesterone to oestrogen should be 600:1 and over to feel well.
Please have a vitamin D test done. For more info on vitamin D levels, test kits etc see...
Blood levels should be 70-100ng/ml or 175-250nmol/L and not the 30ng/ml or 75nmol/L most labs and doctors regard as adequate. The minimum daily dose should be 5000iu's per day, although the latest research indicates it should be 10,000iu's per day, see here.
See the Hormone Testing page for more information on hormone levels.
See here for information on... progesterone testing methods.
The following chart gives an idea of when to use progesterone during a cycle. Bearing in mind if adverse symptoms are experienced, progesterone should be used daily throughout the cycle until symptoms have gone.
Ovulation Chart...
The amount of progesterone to use is dependant on symptoms.
- Follicular phase... This starts on the first day of bleeding and ends at ovulation, no progesterone is used
Luteal phase... This starts from ovulation until bleeding. It is always, in all women, 12-14 days long
Progesterone should be used during the luteal phase.
For contraceptive purposes, deduct 5 to 8 days from the date of ovulation to start progesterone.
Approximate date of ovulation...
|
Cycle length 21 day 22 day 23 day 24 day 25 day 26 day 27 day 28 day 29 day 30 day 31 day 32 day 33 day 34 day 35 day |
Day 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 |
Menstruation should start within a day or two of stopping the progesterone.
Here's a chart comparing ml and teaspoons for a 3.3% progesterone cream...

Having read this you have now learnt pretty much all there is to know about how to use progesterone cream, but please don't forget the important message about...
Do you have a progesterone deficiency?
This free questionnaire
will tell you in 5 minutes.
Just enter your email
and click the button...
Subscribe to our Progesterone Therapy Newsletter
It's free and will bring you important new information on progesterone therapy, related health matters and discount specials.
Do you have a
question or concern?
See what's being discussed, ask for help, give your thoughts or experiences, or just browse...
or
Recent Articles
-
Beyond PCOS: How PMOS Better Explains The Condition
May 19, 26 08:00 AM
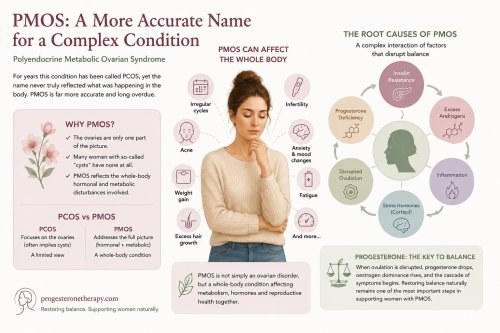 For years this condition has been called PCOS, yet the name never truly reflected what was happening in the body. The ovaries are only one part of the picture. Many women with so-called “cysts” have n…
For years this condition has been called PCOS, yet the name never truly reflected what was happening in the body. The ovaries are only one part of the picture. Many women with so-called “cysts” have n… -
PMOS
May 15, 26 09:51 AM
Polyendocrine Metabolic Ovarian Syndrome (PMOS) -
Contraceptives
May 09, 26 11:11 AM
 Contraceptives are now ubiquitous, reaching even the most remote rural communities. But their widespread use raises an important question—at what cost to a woman’s health? All drug-based contraceptive…
Contraceptives are now ubiquitous, reaching even the most remote rural communities. But their widespread use raises an important question—at what cost to a woman’s health? All drug-based contraceptive… -
Honouring Value: Upcoming Natpro Price Changes
Apr 19, 26 09:34 AM
 We deeply value your trust and loyalty as part of the Natpro community. Over the past 30 years, we have worked hard to keep Natpro’s pricing stable, ensuring the highest quality natural progesterone c…
We deeply value your trust and loyalty as part of the Natpro community. Over the past 30 years, we have worked hard to keep Natpro’s pricing stable, ensuring the highest quality natural progesterone c… -
Hot Flushes, why they happen and how to get relief
Apr 08, 26 04:37 AM
 Hot flushes are the body’s attempt to regulate temperature, a natural response when it senses an imbalance. The skin, being the body’s main defence against overheating, responds with flushing and swea…
Hot flushes are the body’s attempt to regulate temperature, a natural response when it senses an imbalance. The skin, being the body’s main defence against overheating, responds with flushing and swea…
Natural
progesterone cream
Your language
Translate this website
into your language
Is this the future
of medicine?
Home | Contact | Newsletter | Index of Symptoms | News | Progesterone cream | Privacy policy | Blog | About | FAQ
Disclaimer:
Although this web site is not intended to be prescriptive, it is intended, and hoped, that it will induce in you a sufficient level of scepticism about some health care practices to impel you to seek out medical advice that is not captive to purely commercial interests, or blinded by academic and institutional hubris. You are encouraged to refer any health problem to a health care practitioner and, in reference to any information contained in this web site, preferably one with specific knowledge of progesterone therapy.